Blossom Health Data Shows Patients Improve With Each Psychiatric Visit
Author:
Blossom Health Team



For patients managing depression, anxiety, and other mental health conditions, sustained engagement with a clinician is what drives meaningful, lasting improvement in outcomes.
At Blossom Health, our care model is built around this principle. As a psychiatrist-led mental health platform, we connect patients with board-certified providers for virtual, in-network care, matching treatment intensity to clinical need and tracking progress using validated measures at every visit.
Today, we're publishing data that demonstrates the impact of this approach:
68% of depression patients showed measurable improvement in PHQ-9 scores across visits
66% of anxiety patients showed measurable improvement in GAD-7 scores across visits
Patients seen four or more times showed an average depression score drop of 4.6 points and an average anxiety score drop of 4.3 points
Symptoms continued to decline at every visit, not just between the first and second appointments
This data demonstrates the Blossom care model working as designed: matching psychiatric expertise to patient need, driving sustained engagement, and delivering meaningful clinical results.
Key Takeaways
Blossom published data across 8,635 patients and 42,592 assessments, showing that patients who engage consistently with virtual psychiatric care achieve meaningful reductions in depression and anxiety symptoms, with about two out of three patients improving on both standardized measures.
The data shows that patients tracked across four or more visits showed an average PHQ-9 drop of 4.6 points and a GAD-7 drop of 4.3 points, with scores declining at every visit, not just at the start of care.
By delivering consistent, evidence-based care through a telehealth platform covered by in-network insurance, Blossom helps patients achieve lasting improvements in mental health, including concentration, sleep, energy, and anxiety symptoms.
How We Measured Patient Progress
Tracking whether treatment is working requires more than asking patients how they feel. We used two widely accepted, validated clinical tools across every patient visit.
PHQ-9 (Patient Health Questionnaire-9)
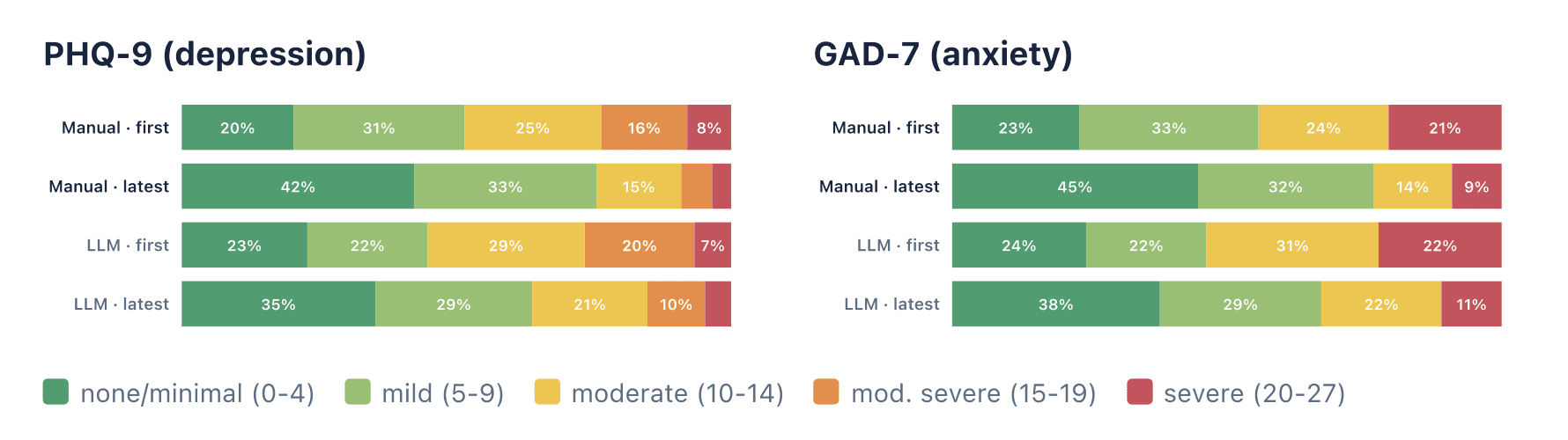
A nine-question screening tool used to measure depression severity on a scale of 0 to 27. Scores of 0 to 4 indicate minimal symptoms, 5 to 9 mild, 10 to 14 moderate, 15 to 19 moderately severe, and 20 or above severe. It is one of the most widely used depression screening instruments in clinical practice.
GAD-7 (Generalized Anxiety Disorder-7)
A seven-question tool that measures anxiety severity on a scale of 0 to 21, with similar severity thresholds. It has been validated as a reliable screener for generalized anxiety disorder and anxiety severity more broadly.
Scores were collected in two ways: through clinician-administered or patient-entered forms, and through structured scoring from visit transcripts when no form was available. Both methods pointed in the same direction.
What the Data Shows
Across 8,635 patients and 42,592 assessments, patients tracked at multiple time points showed consistent improvement on both measures.
Depression Scores (PHQ-9)
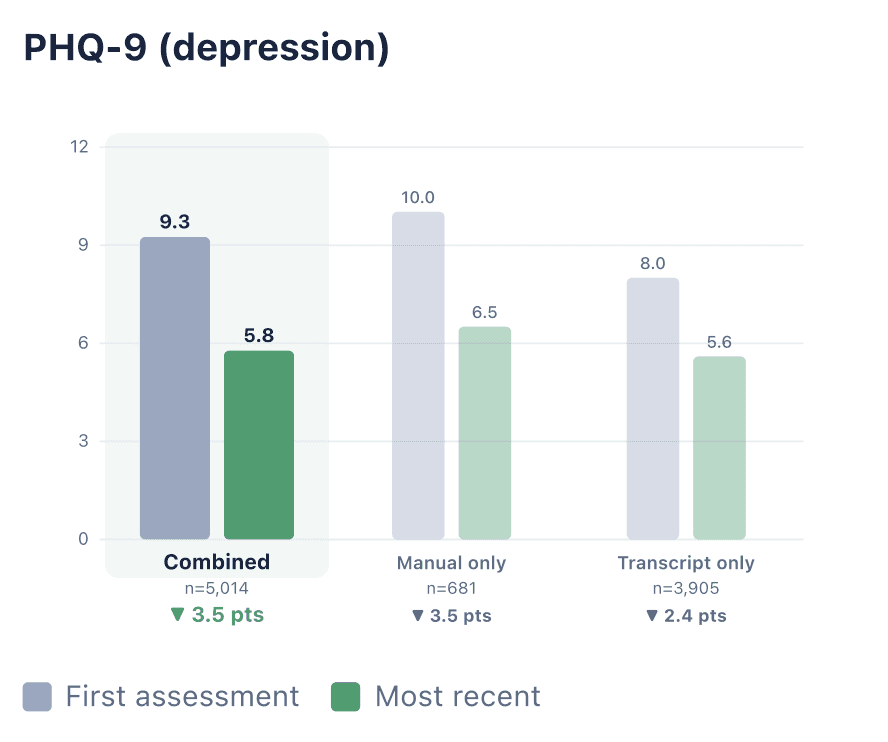
Among 5,014 patients measured more than once, average PHQ-9 scores dropped from 9.3 to 5.8, a reduction of 3.5 points. That shift moves the average patient from the mild range at the start of care toward minimal symptoms over time.
Of patients with complete forms at both a first and follow-up visit, 68% showed improvement. Among patients measured at least four times, the average PHQ-9 score fell from 9.9 to 5.3, a drop of 4.6 points across roughly three months of care.
Anxiety Scores (GAD-7)
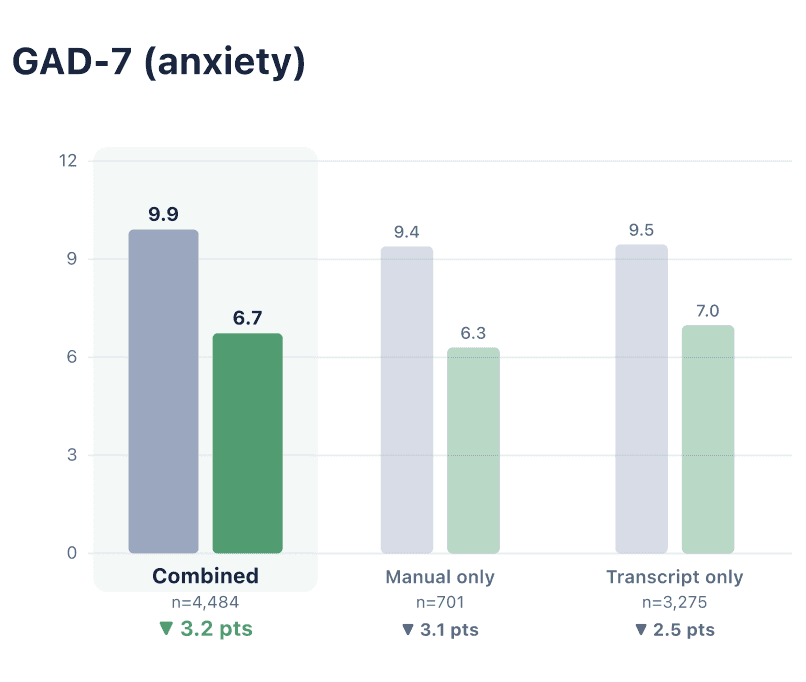
Among 4,484 patients measured more than once, average GAD-7 scores dropped from 9.9 to 6.7, a reduction of 3.2 points. The average patient began care in the moderate anxiety range and moved into the mild range by their most recent visit.
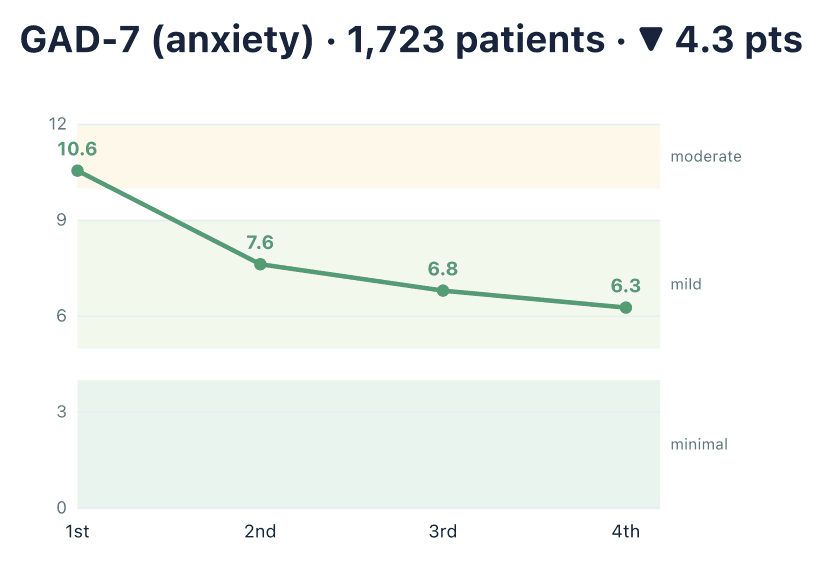
Among patients measured four or more times, scores dropped from 10.6 to 6.3, a reduction of 4.3 points. Sixty-six percent of patients with complete forms showed measurable improvement in anxiety symptoms.
Improvement Held Across Both Measurement Methods
Whether scores came from clinician-entered forms or transcript-derived scoring, the pattern was consistent. Manual-only patients showed a 3.5-point drop in PHQ-9 and a 3.1-point drop in GAD-7. Transcript-scored patients showed drops of 2.4 and 2.5 points, respectively.
Which Symptoms Improved Most
Not all symptoms move at the same pace. Looking at individual PHQ-9 questions, the largest improvements were seen in:
Concentration difficulties (Q7): the most improved item across both measurement methods
Low energy and fatigue (Q4)
Sleep problems (Q3)
Appetite changes (Q5)
Feelings of worthlessness (Q6)
For anxiety, the two most improved items were feeling nervous or anxious and feeling easily annoyed or irritable, each showing meaningful average reductions.
The PHQ-9 question about self-harm thoughts remained very low throughout treatment, both at the start and at follow-up. This is an important safety signal and consistent with what you would expect in an outpatient psychiatric population.
Patients Who Stayed in Care Kept Getting Better
One of the most meaningful findings in this data is that improvement was not a one-time event between the first and second visits.
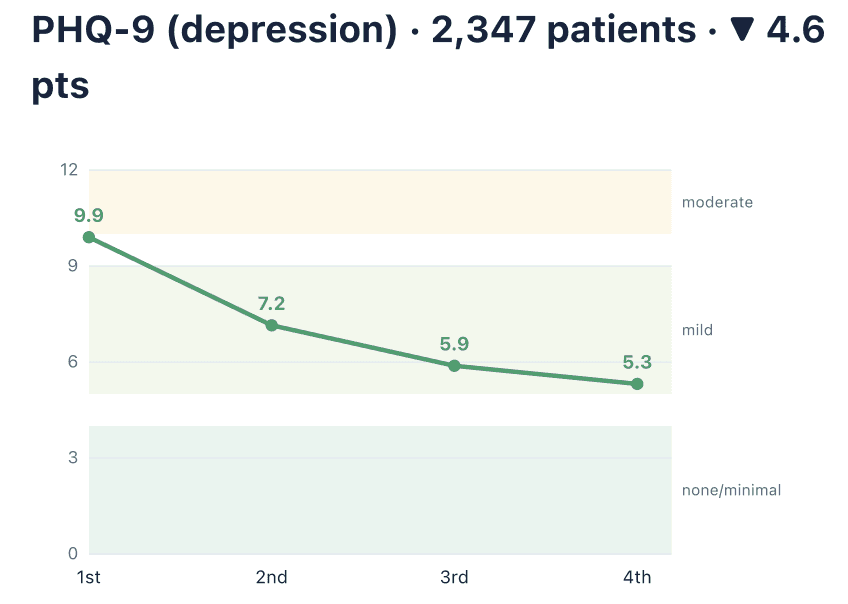
Among patients with at least four assessments spaced roughly a month apart, symptoms dropped at every visit, not just at the beginning of treatment.
For depression, the trajectory was: 9.9 at the first visit, 7.2 at the second, 5.9 at the third, and 5.3 at the fourth.
For anxiety: 10.6, then 7.6, 6.8, and 6.3.
This pattern held whether scores came from manual forms or transcript scoring. It suggests that consistent, ongoing psychiatric care, rather than a single intervention, drives the largest gains over time.
A Note on Methodology
These are real-world outcomes from production data, not a controlled clinical trial. There is no comparison group, and patients choose whether to stay in care. This shows how symptoms moved during treatment. It does not prove that treatment alone caused the change.
For a stricter measure of meaningful clinical change, we also applied the threshold used by the UK's NHS Talking Therapies program: an improvement of 5 or more points on the PHQ-9 and 4 or more points on the GAD-7. By that standard, 39% of PHQ-9 patients and 40% of GAD-7 patients met the threshold for reliable improvement.
What Psychiatric Care at Blossom Looks Like
If you are new to psychiatric care, it helps to know what to expect. At Blossom, care is delivered entirely via video visits and is covered by in-network insurance.
Your first appointment is typically one hour. Your provider will review your symptoms, mental health history, medical background, and current medications, then work with you to build a personalized treatment plan. That may include medication management, therapy recommendations, or both.
Follow-up visits are shorter, usually 15 to 30 minutes, and focus on monitoring your progress and adjusting your treatment plan as needed.
The standardized scores described in this report are part of that monitoring process, providing your provider with a consistent, objective way to measure your response over time.
If you are ready to get started, you can schedule your first appointment.
This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition. If you are experiencing a mental health crisis, contact the 988 Suicide and Crisis Lifeline by calling or texting 988.
















































































































































































































































































